




What is the Best Treatment for Varicose Veins? – Kavic Laser & Vein Center
Which Vein Treatment Works Best for Most people with Varicose veins?
The Best Vein Doctor Discloses the Best Treatment for Varicose Veins

Credit: Society for Vascular Surgery
The answer to this question is from the most respected and experienced (read: best) vein doctor in the world, Dr. Peter Gloviczki.
Dr. Gloviczki was the chief of vascular surgery at the Mayo Clinic and the past president of the Society for Vascular surgery, the most prestigious vein society in terms of rigorous research, patient advocacy, and innovation in the treatment and cure of vascular disease.
He wrote the clinical practice guidelines for the care of patients with varicose veins and chronic venous disease in 2011 which is the foundation for the treatment of varicose veins.
It has been cited a remarkable 703 times by other authors.
This document is used by insurance companies to determine best practices and to determine which therapies are worthy of reimbursement.
Dr. Gloviczki has innumerable additional honors, awards, publications and achievements.
As a vascular surgeon with forty-five years of experience treating the entire spectrum of vascular disease, he also has a special interest in venous disease.
Dr. Gloviczki’s curriculum vitae is over 160 pages long and is extraordinarily impressive.
There’s no vein doctor in the world who comes close to these qualifications!
Incredible!
That’s why when Medicare recently met to discuss the future of coverage of varicose veins, they chose him above all others to testify.
As an analogy, when Congress wants to know the state of the economy, they summon the Chairman of the Federal Reserve to testify.
Here is his response and his recommended treatment for varicose veins in this interview with Dr. Peter Gloviczki, MD FACS.
The Best Treatment for Varicose Veins According to the Best Vein Doctor – Dr. Peter Gloviczki
For those who didn’t read the entire preceding link, this is what Dr. Gloviczki recommends and practices at the Mayo Clinic for his patients with varicose veins.
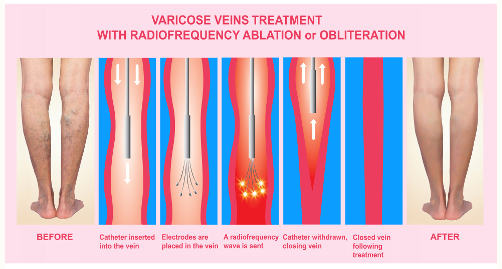
“For treating superficial chronic venous disease, including varicose veins and chronic venous insufficiency, I use percutaneous radiofrequency ablation for saphenous vein ablation and phlebectomy of varicose tributaries.”
I agree.
 For most people with symptomatic bulging varicose veins of the legs, it is also my recommendation that the best treatment for most people’s varicose veins is radiofrequency ablation of the underlying saphenous vein and phlebectomy for the visible large surface veins.
For most people with symptomatic bulging varicose veins of the legs, it is also my recommendation that the best treatment for most people’s varicose veins is radiofrequency ablation of the underlying saphenous vein and phlebectomy for the visible large surface veins.
Often a combination of these last two procedures is necessary for the longest lasting results.
Those two treatments can be staged if the problem is advanced and extensive or combined into one procedure.
However, in less than 10% of people with varicose veins, the saphenous veins are completely normal.
When the saphenous veins are normal, the source or root of the problem is often either the pelvic veins inside of the abdomen or perforating veins.
Perforating veins are short veins that connect the deep veins of the leg with the superficial veins near the surface of the skin.
In this subgroup of individuals, either sclerotherapy (injections) or phlebectomy (removal of the varicose veins through mini incisions) works best.
Again, a combination of these two treatments may be necessary to get optimum long-lasting results.
Why Are Radiofrequency and Phlebectomy Treatments the Best Approach?
From experience, laser for the saphenous veins works as well as radiofrequency but the pain and side effects of laser makes it an inferior choice to radiofrequency. In some cases, laser may be necessary for technical reasons.
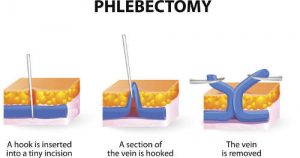 After the abnormal saphenous vein is treated, the largest varicose veins on the surface of the skin (greater than 5 mm in diameter) should be physically removed.
After the abnormal saphenous vein is treated, the largest varicose veins on the surface of the skin (greater than 5 mm in diameter) should be physically removed.
The best way to do that is with phlebectomy as shown on the left.
If a doctor tries to inject these large veins instead, painful clots within the vein last for weeks.
Compassionate vein doctors will bring the patient back about two weeks after the injection treatment to drain trapped blood within these large tender and sometimes very painful veins.
This discomfort after injecting large veins is instantly relieved when the trapped blood is expressed after the overlying skin is numbed and a large needle is inserted into the painful vein.
Old trapped blood is expressed which instantly relieves the discomfort from the previously treated vein.
It’s almost like squeezing a pimple.
Relief is immediate.
Some doctors who perform injections on large varicose veins choose to rarely drain them.
Instead they tell their patients to take anti-inflammatory drugs and use warm compresses.
That’s unnecessarily unkind.
That unnecessary “watchful waiting” approach drags out the discomfort for weeks or longer.
In addition, the brown staining that results after injecting all large veins will continue for a much longer period of time (often over a year).
All of this pain and unsightly brown staining of the skin could have been be avoided altogether by simply doing phlebectomy on these large veins instead of sclerotherapy.
The problem is that many doctors who treat varicose veins have no training or experience with phlebectomy.
That tool is not in their toolbox.
Their patients suffer unnecessarily.
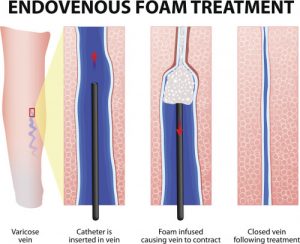
Foam sclerotherapy injections for varicose veins
Another factor to consider is that after injecting foam into large varicose veins, the veins may come back.
It is difficult to get just the perfect concentration of foam in every segment of the varicosities.
Multiple injections are often required with each treatment. As the medicine is injected, the nearby veins go into spasm preventing an even distribution of the medication.
With smaller varicose veins that are more extensive, sclerotherapy may be the better option.
It takes clinical judgement from many years of treating varicose veins to determine which approach is best.
Conclusion
As a vascular surgeon who trained along-side Dr. Gloviczki at the Mayo Clinic, I agree with his approach.
Injecting large varicose veins without these adjunctive treatments results in recurrence within a few years or less.
Dr. Gloviczki stated,
“Patients should be aware that if I use foam [alone], there is a good chance I’ll have to treat you again in the next few years.“
I have used other treatments including Varithena foam, laser alone, and sclerotherapy alone.
I discovered that all of these alternatives provide inferior results and more patient discomfort.
To experience the best approach to treat your varicose veins which is recommended by Dr. Glovikzki, call my office at 724-987-3220 for a consultation to learn more.





{kind=link}